Depression often occurs as a result of adverse life events, such as: the loss of a significant person, object, relationship or health. However, it can also occur due to no apparent cause. These problems can become chronic or recurrent and lead to substantial impairment in an individual's ability to take care of their everyday responsibilities [41]. Depression is a significant public health concern worldwide and has been ranked as one of the illnesses having the greatest burden for individuals, families, and society. In Canada, depression accounts for $14.4 billion annually of health care spending, lost productivity, and premature death. As well, depression is related to increased morbidity and mortality from medical conditions and decreased quality of life among many other negative consequences [1]. A representative randomized sample from 27sites in Dakahlia Governorate (Egypt) shows a prevalence of 10.6% of common mental disorders with significant disability and effect on the QOL. The most frequent diagnosis is the dythymic disorder (3.4%), followed by generalized anxiety disorder (1.7%), major depressive disorder (1.5%) and obsessive compulsive disorder (1.4%) [2]. [3], defined stress, as a nonspecific response of the body to any demand made upon it.
A modern definition of stress is: a psychological and physical response of the body that occurs whenever we must adapt to changing conditions, whether those conditions be real or perceived. Stress has powerful effects on mental functioning, mental and physical performance, interpersonal encounters, and physical well-being [4] showed that chronic stress takes a more significant toll on our body than acute stress does. It can raise blood pressure, increase the risk of heart attack and stroke, increase vulnerability to anxiety and depression, contribute to infertility, and hasten the aging process. [3], says: where stress enhances function (physical or mental, such as through strengthtraining or challenging work), it may be considered eustress. Persistent stress that is not resolved through coping oradaptation, deemed distress, may lead to anxiety or withdrawal (depression) behavior.
The vast majority of research supporting a relationship between stress and depressive episodes has been based on episodic stressors (discrete events that have a beginning and ending) that have negative or undesirable content. There is some evidence of a generally linearassociation between severity and number of negative events and probability of depression onset [5].
Typical symptoms of depression include feeling down for a long time, restlessness, a lack of enjoyment and general lack of interest – even activities that you used to like are no longer enjoyable. Depression sometimes also causes physical symptoms such as tiredness and sleep problems (insomnia). Other problems such as anxiety or pain can arise too. Severe depression is associated with a higher risk of suicide and requires professional treatment. Depression can seriously affect people’s quality of life and often make situations seem hopeless [6].
The most common treatment for depression is medication (antidepressants) or psychological treatment. Many patients are not able to tolerate available antidepressant medications due to side-effects. Studies show that as many as 50% of subjects may discontinue antidepressant treatments within the first six months of therapy, reporting adverse effects as a major reason for discontinuation. Poor adherence to pharmacological and psychosocial treatments for depression, especially in the elderly, is an additional barrier to the effective treatment of patients suffering from depression. Factors linked to this high non-adherence rate amongst the elderly include lack of information and misperceptions about mental illness and its treatment, stigma, lack of family support, cognitive impairment, and poor physician-patient communication or relationship [42].
Relaxation techniques such as progressive muscle relaxation can help relieve mild to moderate depression. But they are not as effective as a particular type of psychotherapy called cognitive behavioral therapy [6]. Many persons with clinical anxiety or depression turn to non pharmacologic and non-conventional interventions, including exercise, meditation, tai chi, qigong, and yoga. There is increasing scientific interest in the potential effectiveness of these interventions for the treatment of anxiety and depression, especially for mild to moderate levels of disorder severity. These interventions have appeal because their use seems unlikely to have severe adverse effects and they are easily available [7].
Most people don’t express their feelings verbally; they tend to repress them, and when they couldn’t express their wishes or desires in acceptable manner, they learn to express them in physiological symptoms. There is a lack of psychological sophistication in people, they think that symptoms are physiological in nature and only physician can treat it. If there is an absence of medical bases then people visit different types of healers who try to treat patients with conventional medicines. There are very few people who visit clinical psychologist for psycho therapy [8], [9], [10]. A lot of empirical work [8], [9], [10] showed that muscle tension is related to anxiety and that an individual will experience comfort and decreased amount of anxiety if tense muscles can be made loose and comfortable. Relaxation is best when used within the context of self-management by the clients. After the therapist has gone through the relaxation protocol two-three times, clients are encouraged to practice on their own, which serve as a mean of coping with stress.
2. Significance of the Study
Depression is a psychological disorder with signs and symptoms such as loss of appetite or overeating, sleeplessness or oversleeping, concentration problems, recurring thoughts of death, sadness or lack of interest, psychomotor retardation, lack of energy and tiredness, feelings of worthlessness and guilt and difficulty making decision. People with depression often struggle with more emotional weight than depression alone. Depression and anxiety often go hand-in-hand, and stress can also challenge your emotional health. When anxiety and stress build up, they can affect your depression symptoms and make them more difficult to manage. Some simple relaxation techniques may help you escape your stress and anxiety, as well as better manage your depression. Reducing depression in depressed patients, can lead to increasing social adaptability. It appears that learning social and communicative skills, problem-solving skills, self-expression skills and emotion control skills such as anger management and relaxation therapy skills play an important role in the treatment of depression [11]. Psychiatric nurses take an active role in reducing stress and anxiety when they are trained in massage and deep breathing techniques they can administer to anxious patients. The role of the nurse at this time is helping to promote the health. Health promotion includes strategies for reduction and management of the stress, the nurse also can use nursing process in order to manage the stress. The nurse should be able to teach individuals to learn how to cope more effectively with stress by providing (1) specific exercises and techniques that inoculate the individual to stress, (2) treatment program to increase social skills and self-esteem and (3) ongoing support groups.
3. Subjects and Methods
3.1. The Aim of the Study
The aim of the study is:-
- The Primary aim is to evaluate the effect of stress management program with depressed patients on stress, anxiety, and depression of depressed patients.
- The secondary aim is to assess the relationships between anxiety, depression and stress.
3.2. Research Hypothesis
Application of stress management program with depressed patients will reduce stress, anxiety, and depression of depressed patients.
3.3. Research Design
Quasi-experimental design (one group pre test-post test design) was used to achieve the aim of the study.
3.4. Research Setting
The study was conducted at The Psychiatric and Addiction Treatment Hospital in Mit-Khalf at Menoufia, Egypt.
3.5. Subjects
-A Purposive sample (30) was selected in the chosen setting outpatient clinics.
3.5.1. Inclusion Criteria
• Patients who were diagnosed by psychiatrists as depressed patient.
• Patient aged from 18- 60 under treatment therapy
• Both sexes.
• Alert and agree to participate in the study
3.5.2. Exclusion Criteria
Patients who were being treated for psychosis, bipolar disorder, or major substance misuse.
3.6. Instruments of the Study
The instrument used to collect the data was the depression, anxiety and stress scale (DASS):
• The depression, anxiety and stress scale (DASS) by (lovibond and lovibond, 1995) translated into Arabic and tested for content validity by (Kotb, 2007). Reliability of three scales is considered adequate and test-retest reliability is likewise considered adequate with .71 for depression, .79 for anxiety, and .81 for stress. It consisted of a 42- questionnaire which includes three self report sub-scales designed to measures the negative emotional states of depression, anxiety and stress. Each of the three sub scales contains 14 items, depression (14 items), anxiety (14 items), stress (14 items) divided into subscales of 2-5 items with similar content. The depression scale assesses dysphoria, hopelessness, and devaluation of life, self- deprecation, and lack of interest, anhedonia, and inertia. The anxiety scale assesses autonomic arousal, skeletal muscle effects, situational anxiety, and subjective experience of anxious effect. The stress scale (items) is sensitive to levels of chronic non- specific arousal; it assesses difficulty relaxing, nervous arousal, and being easily upset, irritable and impatient. Scores for depression, anxiety and stress are calculated by summing the scores for the relevant items .The total score ranges from 14-42. The higher score indicates negative emotional status.
• In addition to socio-demographic data of the patients such as age, sex, occupation, level of education and family history of mental illness, compliance of medication.
3.6.1. Reliability of the Tools
Reliability was applied by the researcher for testing the internal consistency of the tool, by administration of the same tools to the same subjects under similar conditions on one or more occasions. Answers from repeated testing were compared (Test-re-test reliability).
3.6.2. Validity of the Tools
They were tested for content validity by jury of five experts in the field of psychiatric Health Nursing and Pediatric nursing specialty to ascertain relevance and completeness.
3.6.3. Data Collection Methods
Data collection for the study was carried out in the period from October 2013 to December 2013. The researcher collected the data during the morning at two days/week from 10 AM to 12 AM. An official letters were issued from the Faculty of Nursing Menofia University, and send to the directors of The Psychiatric and Addiction Treatment Hospital in Mit-Khalf at Menoufia, Egypt, after explanation of the aim of the study to get their permission. Ethical Consideration: An oral consent was obtained from patients to participate in the study. During the initial interview the purpose of the study was explained. The subjects were assured that all information would be confidential and their participation in the study was voluntary without any costs.
A Pilot study was carried out 5 patients before starting data collection; this was done to estimate the time required for filling out the sheet and also to check the clarity of the tools. The sample of the pilot study was excluded from the study.
3.7. Procedure of Data Collection
The questionnaire used in the study was administered by the researchers. The patients were briefed about the purpose of the study, encouraged to participate and motivated to express their feelings. The patients give fully informed verbal consent to participate. It was emphasized that all data collected was strictly confidential and the data would be used for scientific purposes only. The subjects were divided into 5 groups; each of them consisted of 6 patients. The period of implementation was 2 months.
Implementation of the study passed into three phases (pre assessment phase, implementation phase and post assessment phase).
3.7.1. Pre Assessment Phase (Measure1)
A comfortable, private place was chosen for the interview.
Orientation was done my name, purpose, significance, content. Subjects were interviewed individually at their rooms where pre- assessment was done using the depression, anxiety and stress scale (DASS) and socio-demographic questionnaire.
3.7.2. Implementation Phase
The stress management program aimed at reducing stress, anxiety, and depression of depressed patients.
The stress management group met for eight consecutive weekly sessions that lasted approximately 2 hr. The researcher led the group and the co-leader recorded the sessions. This training program has a set of specific objectives for each of the 8 sessions. This was achieved through several teaching methods such: lectures interweaved with group discussion, brainstorming, and examples from real life, modeling, role playing / behavioral rehearsal, getting participants' feedback, providing feedback, providing corrective feedback, and assigning homework. Each session focused on stress management techniques that could be used in everyday life. One session is lecture on the nature of stress provided by the researcher, seven practice sessions in stress management techniques & relaxation methods and a group discussion of how individuals experience the symptoms of stress, the everyday stressors in their lives and the activities that are useful in controlling stress and the healthy life style.
The content of the stress management program sessions was as follows:
1. Introduction about the concept and nature of stress causes of stress; how individual experience the symptoms of stress; the everyday stressors in their lives.
2. How individual respond to stress.
3. The activities those are useful in controlling stress and the healthy life style.
4. The stress management techniques.
5. How to make progressive muscle relaxation.
6. How to make deep breathing exercises.
7. How to make meditation
A short description of the stress management techniques employed in the study are discussed below.
Progressive Muscle Relaxation (PMR) (Jacobson, 1938)
It is a technique for reducing stress and anxiety by alternately tensing and relaxing the muscles it was developed by American physician Edmund Jacobson in the early 1920s. Jacobson argued that since muscle tension accompanies anxiety, one can reduce anxiety by learning how to relax the muscular tension. PMR entails a physical and mental component. Method/Path physiology: The physical component involves the tensing and relaxing of muscle groups over the legs, abdomen, chest, arms and face. In a sequential pattern, with eyes closed, the individual places a tension in a given muscle group purposefully for approximately 10 seconds and then releases it for 20 seconds before continuing with the next muscle group. The mental component requires that the individual focuses on the distinction between the feelings of the tension and relaxation. With practice, the patient learns how to effectively relax in a short period of time. Therefore, the individual is taught by the researcher, manual or audio how to progressively relax majormuscle groups and performs the sequence 2-3 times daily for 15-20 minutes per session.
Deep Breathing Exercises
Patients are taught by the researcher, manual or audio how to inhale and exhale deeper and slower. They need to practice several times a day, or as needed, for a few minutes to see immediate benefits. Method/Path physiology: - (1) Sit comfortably with your back straight. Put one hand on your chest and the other on your stomach. (2) Breathe in through your nose. The hand on your stomach should rise. The hand on your chest should move very little. (3) Exhale through your mouth, pushing out as much air as you can while contracting your abdominal muscles. The hand on your stomach should move in as you exhale, but your other hand should move very little. (4) Continue to breathe in through your nose and out through your mouth. Try to inhale enough so that your lower abdomen rises and falls. Count slowly as you exhale.
Meditation
Clients were given training on Meditation which involves assuming a comfortable position, closing the eyes, casting off all other thoughts and concentrating on a single word, sound, or a phrase that has positive meaning to the individual. It can be practiced 20 min once or twice daily.
3.7.3. Post Assessment Phase (Measure 2)
Evaluation was done using the depression, anxiety and stress scale (DASS) to assess level of depression, anxiety and stress.
3.8. Data Processing and Analysis
The statistical analysis conducted here was done using SPSS program (Statistical Package for Social Sciences) version 21. The results introduced in this paper are divided into two parts: (1) Descriptive part: - In this part, some descriptive statistics are used to describe sample properties. Since most of the variables in the study are categorical ones (nominal / ordinal), frequency tables are used to give the number of patients in each category and the corresponding percentage to reflect the relative size of each category compared to other categories. For quantitative variables, mean and standard deviations were calculated. (2) Analytical part: -Three scales are calculated, namely, depression, anxiety and stress. To test whether the stress program is effective or not, t test for paired samples is used to test whether there is a significant difference between the mean of depression, anxiety and stress before and after applying the stress program. To investigate the correlations between the three scales and some demographic variables, t tests for independent samples and one way ANOVA F tests were used for qualitative demographic variables. For quantitative demographic variables, Pearson correlation coefficient is calculated to measure the direction and strength of the correlation. The corresponding p-value (significance) of each test is calculated. According to this value the results are determined to be statistically significant or not. Setting the level of significance α =0.05 such that if sig. <α this means that the test is statistically significant, i.e., there is correlation between these variables.
4. Results
Table (1) show that the majority of studied patients (90%) were in age group(30>60) years, 50% had secondary education, 50% were female equal to male, The highest frequency (60%) were married, 50% of them were unemployed, 70% were incompliance on their medication.
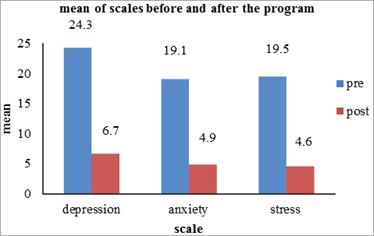
Figure1 illustrated that, there were highly statistically significant difference between pre and post intervention program regarding depression, anxiety and stress score levels.
Table (2) illustrated that there was positive relation between depression, anxiety and stress i.e. when depression increased anxiety and stress increased, while there was positive relation between anxiety and stress but not significant.
Table (3) illustrated that, there was positive significant correlation between age, diseases experience and depression; also there was positive significant correlation between age, diseases experience and anxiety; while there was no significant correlation between age, diseases experience and stress.
Table (4) shows that there were highly statistically significant relations between depression and education, marital status and past history.
Table (5) illustrated that there were highly statistically significant difference between anxiety and education, occupation while there were no statistically significant differences between anxiety and sex, compliance, marital status and past history.
Table (6) show that there were highly statistically significant difference between stress and sex, education, marital status and compliance, while there were no statistically significant difference between stress, occupation and past history.
Table (3). Pearson correlation between age, diseases experience and anxiety, depression and stress of depressed patients.
| Items | Pearson correlation |
| age | diseases Experience |
| r | P-value | r | P-value |
| depression | 0.834 | 0.00 | 0.652 | 0.00 |
| Anxiety | 0.759 | 0.00 | 0.855 | 0.00 |
| stress | 0.222 | 0.239 | 0.130 | 0.495 |
Table (4). Relation between depression and socio-demographic characteristics of depressed patients. (t-test and one way ANOVA F test).
| Item | Depression |
| test value | P-value |
| Sex | -1.11 | 0.27 |
| Education | 360.6 | 0.0 |
| Occupation | 1.968 | 0.159 |
| Marital status | 11.1 | 0.0 |
| Past history | 3.1 | 0.0 |
| Compliance | -1.3 | 0.2 |
Table (5). Relation between anxiety and socio -demographic characteristics of depressed patients (t-test and one way ANOVA F test).
| Item | anxiety |
| test value | P-value |
| Sex | -1.22 | 0.24 |
| Education | 13.2 | 0.0 |
| Occupation | 24.149 | 0.0 |
| Marital status | 1.2 | 0.3 |
| Past history | -0.3 | 0.7 |
| Compliance | 0.2 | 0.9 |
Table (6). Relation between stress and socio -demographic characteristics of depressed patients (t-test and one way ANOVA F test).
| Item | stress |
| test value | P-value |
| Sex | -4.6 | 0.0 |
| Education | 12.5 | 0.0 |
| Occupation | 0.146 | 0.865 |
| Marital status | 94.8 | 0.0 |
| Past history | 1.1 | 0.2 |
| Compliance | -4.3 | 0.0 |
5. Discussion
It is clear that relaxation therapy is effective treatment methods in the reduction of depression and anxiety disorders. In our culture there is a lack of psychological sophistication in people, they think that symptoms are physiological in nature and only physician can treat it. If there is an absence of medical bases then people visit different types of healers who try to treat patients with conventional medicines. There are very few people who visit clinical psychologist for psycho therapy. However, with the advancement of education; now a day’s people have started visiting clinical psychologist and for psychotherapy [15]. This study aimed to evaluate the effect of stress management program with depressed patients on stress, anxiety, and depression.
The results of the present study indicated that, stress management training program had positive reductive effect on stress level of depressed patients. This indicated that the sessions had a positive effect in increasing their ability to relax and in learning to recognize individual stress reactions as well as new alternatives to coping with stress. Moreover the stress management program might helped them to become more aware of thesymptoms of stress, stressors that "trigger" symptoms and everyday activities that can be used to control stress; this result supported by the study of [16] who indicated that stress management training program could have a significant reduction in stress, anxiety and depression level in the intervention group in comparison with the control group and this reduction was also significant in the follow-up step.
The present study revealed that anxiety level of depressed patients had reduced through implementing stress management training program; this could be as a result of a psych educational approach which taught them to control anxiety, to increase the ability to problem solve, to learn how to relax, and to cope more effectively with stress; this result supported by [15] indicated that there was a reduction in anxiety related symptoms after applying the relaxation therapy ,which included deep breathe, simple muscle relaxation, involving in recreational activities, going on vacations, managing time, and visualization, also [17] revealed that practicing deep breathing exercise daily for 2 weeks 2 times a day for 10 min has significantly decreased the anxiety level and diastolic blood pressure of patients with CAD. Moreover [10] investigated the efficacy of worry exposure and applied relaxation therapeutic techniques for the treatment of generalized anxiety disorder, while comparing with control group both were found to be effective.
This study indicated that depression level of depressed patients had reduced through implementing stress management training program this could be due to effect of stress management training program in increasing their ability to react and deal with stressful situations, to relax and learn new alternatives to coping with stress as increase the ability to problem solve and learn how to relax. this result consistent with The results of [18];titled as "reviewing the effectiveness of stress management training on blood sugar and depression of patients with type II diabetes" indicated that stress management training program could reduce the depression mean score of the patients in the follow-up step, which this reduction was significant as compared with the control group.
Also the study results of [19] titled as "How stress management improves quality of life after the treatment for breast cancer" showed that depression level of the women with breast cancer had reduced in the intervention group in the follow-up step and this reduction was significant as compared with the control group. Moreover, the result of [19], [20], [16], [18], studies that all of them have approved the efficacy of cognitive and behavioral stress management on reducing the depression.
The current study revealed that there were no significant relation between depression and sex this may be due to decrease sample size; contradict to this result [1]who found that Women suffer more from both types of depression than men. Concerning occupation as a factor in depression, the result of the present study showed that this variable had no significant difference. This result disagreed with the finding of [21] where the study showed significant differences in HADS-A and HADS-D scores between major and between sub major occupational groups. Elementary occupations consistently showed ‘higher’ depression.
This study showed that there was highly statistically significant relation between depression and education this result supported by [1] who found that respondents whose education level was less than secondary school have the lowest rate of lifetime depression (9.1%); and the highest rate of lifetime depression (13.4%) is seen among those with "other post-secondary" education. In other hand this result is on the same line with [22] who reported that low educational levels were significantly associated with depression. Higher educational level seems to have a protective effect against depression, which accumulates throughout life. Also [23] found that low educational levels were associated with increased risk for high depressive symptoms.
The results of the present study shown there was highly statistically significant relation between depression and marital status this may be due to lack of communication, difficult financial status, higher expectation from their partner and sexual incompatibility; the result of present study was supported by[1]who found that the relation between depression and marital status is highly significant. The highest rates of lifetime and 12-month depression are seen in divorced and separated respondents, respectively. The lowest rate for both types of depression is seen among married people. The present study showed that there were highly statistically significant relation between depression and Past history this could be due to co morbidity, ineffective life style.
The currents study showed that there was highly statistically significant relation between depression and age; this may be due to life pressure that person faces throughout his life and Stressful life events; while, [1] found that the prevalence of both types of depression increases with age to the highest level for 20 to 24 year olds and then decreases steadily to its lowest level for the participants aged 75 years and over.
The result illustrated that there was positive relation between depression and anxiety such as when depression increased anxiety increased. This result supported by [21] who revealed that Levels of anxiety and depression were investigated simultaneously, which is important because of the high correlation between anxiety and depressive symptoms.
The present study revealed that there were positive significant correlation between age and anxiety this indicated that when age increase, anxiety will increases; this may be due to the challenges and life pressure that person faces throughout his life and Stressful life events; while [24] stated that; adolescents are most prone to anxiety at an early adolescent period between the ages of 11 and 18.It is the period of adolescence when the person experiencing the most challenges in life is inexperienced and highly exposed to peer influence, family and life pressure. Contradict to this result a study that performed by [25] demonstrated that, there was no significant relationship between age and anxiety among aboriginal Fijians peoples from 18-45 years. Also, similar finding was reported by [26] on the relationship between age and anxiety. Moreover, the result in a study performed by [27] showed that there is no significant relationship(r = -.006, p>.05) between age and anxiety among Iranian adolescent students in Tehran’s secondary schools.
This study revealed that there were highly statistically significant difference between anxiety and education (this means that when educational level increase the anxiety will increase); this may due to educated people able to solve and cope with the problems than non-educated so, the level of anxiety decreased. This result is on the same line with [22] who reported that Low educational levels were significantly associated with anxiety. Higher educational level seems to have a protective effect against anxiety, which accumulates throughout life. Also [23] found that Low educational levels were associated with increased risk for high depressive and anxious symptoms.
This study revealed that there were no statistically significant differences between anxiety and sex; this may be due to decrease sample size in this study; this result was supported by [28] showed, there is no significant difference in levels of test anxiety between male and female students. Also the result of t-test analysis in a study that performed by [29] was demonstrated, there is no significant difference in cognitive test anxiety (CTA) level between male and female students. Contradict to this result [30], reported that although females experience higher levels of anxiety, they also score significantly higher than males on cognitive and somatic subscales of the BAI. Also, the result of this study contradicts the findings of [31], who concluded that girls have a higher tendency to acquire psychological disorder than boys.
This study revealed that there is no statistically significant difference between anxiety and marital status. This may be due to decrease sample size in this study. Contradict to this result [32], who revealed that Marriage (versus never married) was associated with reduced risk of first onset of most mental disorders in both genders (anxiety disorder). Also in ref. [33] revealed that the prevalence of anxiety disorders was highest in people who were widowed, separated or divorced (19.0%) and lowest in those who were married.
The result of the present study show that there were highly statistically significant relation between stress and sex; this may be due to gender differences in physiological hyper arousal, catastrophic cognitions and a general level of anxiety in a non-clinical population this result agreement with [34] who found that the prevalence of psychiatric disorders among Iranian women is much higher than among men. Also, recent estimates suggest that approximately 50% of the 70-million Iranian populations consist of women under psychic, social and family pressure [35]. Contradict to this result [36], indicated that results of Spearman's correlation coefficient showed that relationship between sexes and stress not significant. This means that relationship between sex and stress is random
Regardingmarital status the present study revealed that there were highly statistical significant relation between stress and marital status; this may be due to married women over loaded than single, agreement to this result [37] who found that working married women have to face more difficulties in their lives like they experienced more stress and depression as compared to non-working married women. It concluded that on some aspects working married women cannot contribute significantly for the well being of their family. Their attention diverted because of working in two situations. They cannot give proper attention to their marital lives and this causes depression and stress. The present study revealed that there was highly statistical significant relation between stress and compliance; this may be due to when the patients complained with their medication, stress decreased.
This study indicated that there were no statistically significant difference between stress and age; this may be due to decrease sample size, agreement with this result [36], indicated that results of correlation coefficient showed that relationship between age and stress not significant. This means that relationship between age and stress is random. Regarding education the present study revealed that there was highly statistical significant relation between stress and education; this may be due to the educated people able to solve and cope with the problems than non-educated. This result supported by [38], who indicated that education appear to play a role in reported wellbeing with a higher education and associated with higher levels of wellbeing while those with lower levels of education reported significantly more perceived stress when compared to the general population.
The result of the present study reveals that there were no statistically significant difference between stress and occupation this may be due to decrease sample size in this study. Contradict to this result [39], who illustrated that; there are some occupations that are considered more high risk for stress, and that's what we call occupations that cause job strain. And that basically combines occupations that have high psychological demand combined with low control over their environment and over decision-making like a cashier or like a telephone operator.
6. Conclusion
Implementation of stress management program including (progressive relaxation, diaphragmatic breathing, meditation …. .) has a positive effect on reducing stress, anxiety, and depression.
Recommendation
Based on the results of this study we recommend use of stress management program for inpatients with depression and inpatient education for caregiver to encourage patient to use it in home.
References
- Noori Akhtar-Danesh and Janet Landeen. Relation between depression and socio demographic factors. Int. J. Ment. Health Syst. 2007; (1) 4.
- El-Wasify, Mahmoud A.; El-Boraie, Osama A.; El-Atrony, Mohammed H.; Abdel-Fatah, Abdel-Hady G, et al. The Prevalence and Correlates of Common Mental Disorders in Dakahlia Governorate (Egypt). Egypt. J. Neuro. Psych. Neurosur. 2011; 48: 4: 375 -381.
- Ahmadvand, M. A. Mental health (ed.8). Tehran: Payame-Noor publication. 2010.
- MarinMF, Lord, C, Andrews, J, Juster RP, Sindi, S. h, Arsenault-Lapierre, G., Fiocco, A. J, Lupien, S. J. Chronic stress, cognitive functioning and mental health. Neurobiologyof Learning and Memory. 2011; 96(4):583-595.
- Hammen C. Stress and depression. Annu Rev Clin Psychol. 2005; 1:293-319.
- Institute for Quality and Efficiency in Health Care (IQWiG). Depression: Can relaxation techniques help? 2012.
- Syatezaz, S., Diana, J. Antonacci, and Richard. Exercise, Yoga, and Meditation for Depressive and Anxiety Disorders. Am. Fami. Phys. 2010; 81(8):981-986.
- Conrad, A., & Roth, W. Muscle relaxation therapy for anxiety disorder: It works but how? J.Anxi. Dior.2007; 21(3):243-64.
- Elizabeth A. G., & Doil D. M. A Cognitive-Behavioral, Biofeedback-Assisted Relaxation Treatment for Panic Disorder With Agoraphobia. Nova Southeastern University, Center for Psychological Studies. Clinical Case studies (2006); 5(2), 112-125.
- Hoyer, J., Beesdo, K., Gloster, A. T., Runge, J., Hofler, M., & Becker, E. S. Worry Exposure versus Applied Relaxation in the treatment of generalized anxiety disorder. Psycotherpsychosom; 2009; 78(2):106-115.
- Farahzad A, Arash N, Sayyed D, MeftaghG. G and Hamid A. The effect of stress management training on stress and depression in women with depression disorders: Using cognitive-behavioral techniques.J. Educ.Heal. Prom.2014; 3: (70).
- Lovibond, S. H. &Lovibond, P. f. Manual for the Depression Anxiety Stress Scales. (2nd Ed) Sydney: Psychology Foundation. 1995.
- Kotb F. Social support, psychological distress and suicidal tendency of depressed patient. Unpublished master thesis. Faculty of nursing, Cairo University. 2007:170-172.
- Jacobson E. Progressive relaxation. Chicago: University of Chicago Press. 1938.
- Uzma A., and Shazia H. The Effectiveness of Relaxation Therapy in the Reduction of Anxiety Related Symptoms (A Case Study). Inter. J. Psyc. Stud. 2010; 2(2):202.
- Mehrabi A, Fati L, Davazdah Emami MH, Rajab A. Effectiveness of stress management training based on the theory of cognitive - behavioral control blood sugar and reduces the emotional problems of patients with type 1 diabetes. Iran. J. Diabet. Lipid. 2009; 8(2):103–14.
- Fatima D'silva, Vinay H. & Muninarayanappa N. V. Effectiveness of deep breathing exercise (DBE) on the heart rate variability, Bp, anxiety & depression of patients with coronary artery disease. Nitt. Univ. J. Heal. Scie. 2014; 4 (1), 2249-7110.
- Davazdahemami MH, Roshan R, Mehrabi A, Atari A. Stress Management Training Effectiveness of cognitive - behavioral and depression on glycemic control in type 2 diabetic patients. J. Endocr. Metabo. Iran, Medi. Scie. Healt. Servic. Martyr Beheshti. (2009); 11(4):385–92.
- Antoni MH, Lechner SC, Kazi A., Wimberly, S. R., Sifre, T. Urcuyo, K. R, et al. How stress management improves quality of life after treatment for breast cancer. J Consult Clin Psychol. (2006); 74(6):1143–52.
- Sajadinejad M, Mohammadi N, Taghavi MR, Ashjazadeh N. Effect of cognitive group therapy - treatment of depression and feelings of disability from headache in patients with migraine and tension headaches. Iran. J. Psyc. Clin. Psych. (2008); 14(4):411–8.
- Sanne, B., Mykletun, A., Dahl, A. A., Moen, B. E., Tell, G. S. Occupational Differences in Levels of Anxiety and Depression: The Hordal and Health Study. 2003; 45:6: 628-638.
- Bjelland, I., Krokstad, S, Mykletun A, Dahl A. A, Tell, G. S, Tambs, K. Does a higher educational level protect against anxiety and depression? The HUNT study. 2008; 66(6):1334-45.
- Rebecca C. T, Laura d. K, Ichiro, Kand LISA F. B. Do Depression and Anxiety Mediate the Link Between Educational Attainment and CHD? Psychosomatic Medicine. 2006; 68:25–32.
- Healy, D. Psychiatric Drugs Explained, Section 5: Management of Anxiety, Elsevier Health Sciences. 2009; 136-137.
- Mores, Z., Takau, A. F. Dental Anxiety in Fiji. Pacific Public health. 2004; 11 (1):22-25.
- Mckinley, Sh., Stein-Parbury, J., Chehelnabi, A. Assessment of Anxiety in Intensive Care Patients by Using the Faces Anxiety Scale. Am. J.Crit. Care. 2004; 13(2), 146-152.
- Tabrizi. E. A, Abu Talib. M, Yaacob. S. N. Relationship between creative thinking and anxiety among adolescent boys and girls in tehran. iran, Inter. J. Human. Soci. Sci. 2011; 1 (19).
- Oludipe, B.D. Influence of test anxiety on performance levels on numerical tasks of secondary school physics students. Acad. Lead. onli. J. 2009. 7 (4).
- Faleye, B. A. Cognitive test anxiety and learning outcomes of selected undergraduate students, The African Symposium. 2010; 10 (2), 69-74.
- McIntyre, N., &Roggenbuck, J. Nature/person transactions during an outdoor adventure experience: A multi-phasic analysis. J. Leis. Res. 2006; 30(4): 401-22.
- Esfandyari, B., Baharudin, R., and Nowzari, N. The relationship between inter-parental conflicts and internalizing behavior problems among adolescents. Euro. J. Soci Scie. 2009; 10(4): 641-648.
- Scott, K., Wells J. E, Angermeyer M, Brugha T. S, et al. Gender and the relationship between marital status and first onset of mood, anxiety and substance use disorders. Psychol Med. 2010; 40(9):1495-505.
- The Mental Health of Australians. Anxiety Disorders in Australia. The Mental Health of Australians. 2007; 2 (23).
- Atef Vahid, M. K. Epidemiology of mental disorders in high-school students in Rahfsanjan. Ira. J. Psyc. Clin. Psyc. 2005; 11(1):40, 62-70.
- Farahani, H. A. Comparing Anxiety, Depression and Sexual Life Satisfaction in Two Groups of Fertile and Infertile Women in Tehran. J. Repro. Infer. 2006; 12(4): 2.
- Mostafaei, A. The relationship between stress and mental health in university students. Scholars Research Library: Annals of Biological Research.2012; 3 (7):3468-3473.
- Nagaraju, B., Nandini H. P."A Factor of Marital Status Highly Influencing on Stress of Women Employee’s." A Case Study at Insurance Sector. Inter. J. Busi. Manag. Inven. 2013; 2:10.39-46.
- The Australian Psychological Society Stress and wellbeing in Australia. A state of the nation survey Contact details: Lynne Casey PhD MAPS in 2011.
- Kim L. What Is The Relationship Between Work And Stress? Director, Behavioral Medicine & Psychologist, Northwestern Memorial Hospital. 2008.
- WHO. Depression: A Global Public Health Concern. 2012. Available at:http://www.who.int/mental_health/management/depression/who_paper_depression_wfmh_2012.pdf. Last accessed 16 January 2013.
- WHO. ICD-10. International Statistical Classification of Diseases and Related Health Problems 2010 -10th Revision. Available at: http://apps.who.int/classifications/icd10/browse/2010/en. Last accessed 21 January 2013.
- Gartlehner G et al. Discontinuation rates for selective serotonin reuptake inhibitors and other second-generation antidepressants in outpatients with major depressive disorder: a systematic review and meta-analysis. Int. Clin. Psychopharmacol, 2005, 20(2):59-69.
 (M. I. E. Malky)
(M. I. E. Malky)  (M. M. Atia)
(M. M. Atia)  (S. H. El-Amrosy)
(S. H. El-Amrosy)