Kangaroo Care: Effect on Physiologic Measurements and Physiologic Responses to Pain of a Heel Stick in Pre Term Neonates
Jaklein R. Younis1, Naglaa F. Mahmoud2
1Paediatric Nursing Department, Faculty of Nursing, Menoufia University, Shebin El-Kom, Egypt
2Paediatric Nursing Department, Faculty of Nursing, Cairo University, Cairo, Egypt
Email address

(J. R. Younis)
Citation
Jaklein R. Younis, Naglaa F. Mahmoud. Kangaroo Care: Effect on Physiologic Measurements and Physiologic Responses to Pain of a Heel Stick in Pre Term Neonates. Journal of Nursing Science. Vol. 2, No. 2, 2016, pp. 7-14.
Abstract
Background: Pain in neonates can be associated with various risks. So, it seems essential to find a simple and acceptable method for relieving pain. Pharmacologic agents are not recommended in neonates for pain relief in minor procedures but non pharmacologic interventions like Kangaroo Care (KC) is found to be effective. Aim: this study is a quasi-experimental research design aimed to assess the effect of MKC on physiologic measurements and physiologic responses to pain of a heel stick in preterm neonates. Subject & Methods, this study was conducted at Shebin El Kom and Cairo University hospitals. Forty five pre term neonates who were available at the time of data collection and meet the criteria for sample selection were included. Tools of data collection. Tool one: Biosocial Characteristics of Neonates: It included Sociodemographic characteristics of neonates and their physiological assessment records. Tool two: Neonatal pain assessment scale: is a behavioral scale composed of six indicators. Facial expression, cry, breathing patterns, arms, legs, and state of arousal. Results: The results of this study showed highly statistical significant differences between preterm neonates who were in incubator care group and pre term neonates who were in kangaroo care group regarding their physiological measurements (pulse & respiration) and their total pain response score post painful procedure where (p < 0.001). Conclusion: Kangaroo care had a highly significant effect on neonatal physiological measurements and physiological response to pain. Recommendation: Kangaroo care should be provided as a routine daily care for all neonates in NICUs du to its magic effect on infants’ physiological measurements and their physiological responses to pain.
Keywords
Preterm Neonates, Kangaroo Care, Physiological Response and Pain
1. Introduction
Preterm and sick full-term neonates admitted to the neonatal intensive care unit (NICU) are routinely subjected to many invasive diagnostic and therapeutic procedures which are associated with pain [1]. The heel-lancing procedure is the most common tissue damaging procedure that premature neonates undergo. In the NICU, preterm neonates are subjected to an average of 10 to 16 painful invasive procedures per day with repeated heel sticks accounting for 55% to 86% of these procedures [2]. Pain is a major public health concern throughout the world [1]. Alleviation of pain is a human right regardless of age. Prevention and alleviation of pain is important not only because of being an imperative issue but also because of potential deleterious effects of repeated painful exposures [10]. [11-13].
The deleterious effects of pain in neonates are fairly well described. They include physiological and metabolic effects such as vital signs changes, alteration in cerebral blood flow, and outpouring of stress hormones [5]. Repetitive painful stimuli have been associated with behavioral and emotional problems during later childhood [6]. Despite the increased knowledge of physicians and caregivers regarding neonatal pain, 40% to 90% of neonates do not receive preventive and/or effective treatment to reduce procedural pain [7-9].
Research evident that, newborns are able to feel and remember pain [4]. Therefore, it is important that pain-related stress in preterm and full term neonates is accurately identified, and appropriately managed [27]. Topical anesthetics and opioids are not used to treat procedural pain in newborns because their safety has not been established [44]. Giving sucrose is the most frequently used nonpharmacologic intervention; however, there was a correlation between the prolonged administrations of sucrose during the first week of life and lower neurodevelopment score at the corrected age of 40 weeks in preterm neonates < 31 weeks of gestation [37,38]. Also, breastfeeding during painful procedures was found to be effective for pain control in full-term neonates [32]. However, breastfeeding is not always feasible in preterm neonates. Meanwhile there was an intense need for simple and safe nonpharmacologic method with an analgesic effect for premature neonates. KC was seen as a nonpharmacologic pain relief method for pre-term and full term neonates [17, 18].
Maternal Kangaroo Care (MKC) is a caregiving modality that has been used to enhance the stress regulatory capacity of stable ill newborns [14] and it is now being tested to relieve procedural pain in neonates. MKC is defined as a naturalistic, multilevel intervention consisting of kangaroo positioning, breastfeeding, discharge and follow up care [15].
Many benefits of MKC have been reported [16]. It is thought that kangaroo positioning improves infant physiological stability, thermal regulation and that being held upright exposes the infant to combinations of sensory stimulation (kinesthetic tactile auditory, olfactory, visual and vestibular) [17, 18]. Researchers suggested that, MKC can applied as a non-pharmacological approach to treat procedural pain in premature and full-term newborns but, further information is still required concerning its effect on pain relief and physiological stability in neonates [20]. So, the present study was conducted to assess the effect of MKC on physiologic measurements and physiologic responses to pain of a heel stick in pre- term neonates.
1.1. Aim of the Study
The aim of the current study was to assess the effect of maternal kangaroo care on physiologic measurements and physiologic responses to pain of a heel stick procedure in pre-term neonates.
1.2. Research Hypothesis
Pre term neonates who exposed to maternal kangaroo care during heel stick procedure will show better physiologic measurements and better physiologic responses to pain than pre term neonates in incubator care group.
2. Methods
2.1. Research Design
A quasi experimental design was used for this study.
2.2. Settings
This study was conducted in the NICUs at the following settings:-
1. Menoufia University hospital at Shebin El-Kom city
2. Pediatric hospital- Cairo University
2.3. Sample and Sampling Technique
Forty five pre term neonates who were convenient at the time of data collection and meet the criteria for selection were included. A number of twenty –five preterm neonates were obtained from Menoufia University hospital at Shebin El-Kom town. Twenty preterm neonates were also obtained from Pediatric hospital Cairo University.
Inclusion Criteria
1. Weight ranged from 1.5 Kg - 2.5 Kg and
2. Gestational age was 30 weeks to 36 weeks of gestation, 7-15 days after birth
3. Medically stable and free from any congenital anomalies
4. Not receiving any analgesics within the previous 24 hours
2.4. Tools of Data Collection
Two tools were developed by the researcher for data collection after a review of past and current literature.
Tool One: Biosocial Characteristics of Neonates
It divided into two parts.
Part one:-
Sociodemographic structured questionnaire: It included questions about name, age, sex, gestational age, birth weight, actual weight and type of delivery.
Part two:-
Structured physiological measurements assessment records. It included daily records of Physiological measurements such as respiration, and pulse pre and post painful procedure.
Tool Two: Neonatal Pain Assessment Scale
The Neonatal Infant Pain Scale (NIPS) is a behavioral scale and can be utilized with both full-term and pre-term infants. The tool was adapted from the CHEOPS scale and uses the behaviors that nurses have described as being indicative of infant pain or distress. It is composed of six (6) indicators.
1. facial expression
2. cry
3. breathing patterns
4. arms
5. legs
6. state of arousal
Each behavioral indicator is scored with 0 or 1 except "cry", which has three possible descriptors therefore, being scored with a 0, 1 or 2. Total pain scores range from 0-7. The suggested interventions based upon the infant’s level of pain are listed below.
| Pain Level | Intervention |
| 0-2 = mild to no pain None | None |
| 3-4 = mild to moderate pain | Non-pharmacological intervention |
| with a reassessment in 30 minutes |
| >4 = severe pain | Non-pharmacological intervention |
| and possibly a pharmacological |
| intervention with reassessment in 30 minutes |
2.4.1. Reliability of the Tools
The reliability of the tool was computed using split-half method (r=0.88). This method was used to assess the homogeneity of the tool.
2.4.2. Validity of the Tools
Tools were reviewed by four experts in the field of pediatric nursing and pediatrics (three pediatric nursing experts and one pediatrician).
3. Data Collection Methods
Data was collected at the first of January 2015 to the end of March 2015.
An official permission to carry out the study was obtained from the director of each setting after submitting an official letter from the Dean of the Faculty of Nursing at EL- Menoufia Universityand and Vice Dean for post graduates studies and researches Cairo University explaining the purposes of the study and methods of data collection.
Ethical Consideration: For ethical considerations an oral and written consent was obtained from mothers to share in the study. Therefore, nature of the study, the objectives, its importance safety and confidentiality were explained. Mothers were informed about the privacy of their sessions, and their right to withdraw at any time.
3.1. Pilot Study
A Pilot study was carried out on five pre term neonates (10% of the total sample) to test the clarity and applicability of the tools. No modifications were done. So, the pilot study sample was included in the total sample of the study.
3.2. Procedure of Data Collection
3.2.1. Assessment Phase
Data collection was started on the first of January, 2015 and lasted until the end of March 2015. Data about physiological measurements (pulse & respiration), were collected for all studied neonates.
3.2.2. Implementing Phase
All neonates who were available and meet the criteria for sample selection were demonstrated kangaroo care session separately. Neonates who were demonstrated painful heel stick procedure in incubator during the first day of data collection also demonstrated painful heel stick procedure while in maternal kangaroo care session during the second day. So, the comparison was done among two groups (incubator care group and kangaroo care group) for the same neonates. The procedure lasted thirty minutes for each neonate.
Conducting kangaroo care sessions:
The kangaroo care neonates who received the kangaroo care sessions were allowed twenty five minutes for MKC session. Ten minutes before painful procedure (heel stick procedure) and five minutes during painful procedure (conducting phase) then, ten minutes after it (recovery phase) plus the first five minutes for collecting basic data in the incubator for the two studied groups that assume thirty minutes for total procedure. Each mother conducted kangaroo care sessions separately. During the session each mother had to use two comfortable chairs to extend her legs and recline her back. Newborns were placed between mother’s breasts skin to skin contacts. Neonates had to be facing their mothers and covered with a sterile gown on their back to protect them from any air drafts and maintain their normal body temperature. At the end of each session neonates were carried and received gently. For each neonate, secure all tubes and lines were done. Any required care was provided prior kangaroo care sessions to avoid interruption. Also, oxygen saturation, respiratory rate, heart rate, and temperature were assessed before transfer neonates from incubator to mother to ensure their medical stability.
Procedure:
At 10 a. m. on the first day of study, all of the convenient studied neonates were allowed 30 minutes for conducting the heel stick procedure. Baseline data collection started and continued for five minutes for each group such as physiological measurements (pulse & respiration) and actual weight. Infants in KC group were given to their mothers for 10 minutes before exposure to painful procedure and infants in incubator care group were left in the incubator. Then the Heel (Warming phase, 2 minutes) long, took place, followed by a heel stick to collect blood for lab tests required daily (conducting phase, 3 minutes) and the neonatal responses to pain were assessed during this phase by using neonatal pain assessment tool. Recovery phase began immediately after the heel stick site had been covered with a sterile dressing and continued for 10 minutes. At the end of the Recovery phase, all data collection ceased and the KC infant was placed back in the incubator. Infants already in the incubator were left there throughout all phases. On the second day, the procedure was the same except that infants who had been in KC on the first day were in the incubator on the second day and first day incubator infants were in KC on the second day.
3.2.3. Reassessment Phase
After each session and during the recovery phase, each neonate was reassessed for physiological measurements (pulse & respiration).
3.3. Statistical Analysis
The data collected were tabulated & analyzed by SPSS (Statistical Package for the social Science Software) statistical package version 20 on IBM compatible computer. Quantitative data were expressed as mean & standard deviation (X±SD) and analyzed by applying student t-test for normally distributed variables. Qualitative data were expressed as number and percentage. It was and analyzed by using chi-square test (χ2) for 2X2 table. Pearson correlation was used for explaining relationship between normally distributed quantitative variable and Spearman correlation was used for explaining relationship between normally distributed quantitative variable.
4. Results
Table 1: illustrates socio-demographic characteristics of the studied sample. As shown in this table, the highest percentage of the study subjects (62.2%) were male. The mean gestational age was (34.5 ± 1.14). Regarding, mean birth weight and mean actual weight of the studied sample (2.03 ± 3.6) and (2.13 ± 3.4) respectively. As noticed from this table, (48.9%) had normal delivery and (51.1%) had Cesarean.
Table 2 Distribution of neonatal pain responses levels. This table showed that, the highest percentage of the neonates (40.0% & 55.6%) in kangaroo care group demonstrated no pain, and mild to moderate pain respectively compared to (73,3%) of neonates in incubator care group demonstrated severe level of pain. Also, there was highly statistical significant differences were found between kangaroo care group and incubator care group concerning their total pain response score where (p < 0.001).
Table 3 Distribution of neonatal pain response parameters. This table indicated that, highly statistical significant differences were found between incubator care group and kangaroo care group concerning cry response and their state of arousal where (p < 0.001). Also, statistical significant differences were found between two groups regarding their breathing pattern, arms, and legs movements where (p < 0.05).
Table 4 clarified Spearman correlations between total pain score with sex and types of delivery of the studied neonates It was clarified that, statistical significant difference was found regarding neonatal sex in Kangaroo care group where p (<0.05) and (r =.302).
Table 5 clarified Spearman correlations between total pain score and demographic characteristics of the studied neonates This table showed that, no statistical significant differences were found between total pain score of studied neonates and their gestational age, birth weight and actual weight.
Figure 1, 2: demonstrates distribution of Physiological measurements of studied groups. As indicated by these figures, there were highly statistical significant differences in pulse and respiration rates post exposure to painful procedure between incubator care group and Kangaroo care group where (p < 0.001)
Table 1. Distribution of Socio-demographic characteristics of the studied sample.
| Demographic data | No=45 | % |
| Sex | | |
| Male | 28 | 62.2% |
| Female | 17 | 37.8% |
| Gestational age | | |
| 30 < 34 | 3 | 6.7% |
| 34 -36 | 42 | 93.3% |
| X ± SD | 34.5± 1.14 |
| Birth weight | | |
| 1.5 < 2.0 Kg | 24 | 53.3% |
| 2.0 < 2.5 Kg | 21 | 46.7% |
| X ± SD | 2.03±3.6 |
| Actual weight | | |
| 1.5 < 2.0 Kg | 15 | 33.3% |
| 2.0 - 2.5 Kg | 30 | 66.7% |
| X ± SD | 2.13 ± 3.4 |
| Type of Delivery | | |
| Normal | 22 | 48.9% |
| Cesarean | 23 | 51.1% |
Table 2. Distribution of neonatal pain response levels in Incubator care group and Kangaroo care group.
| Neonatal pain response levels | Incubator care group
no=45 | Kangaroo care group
no=45 | χ2 | P-value |
| No | % | No | % |
| Total pain response score: | | | | | | |
| 0-2 = mild to no pain | 3 | 6.7% | 18 | 40.0% | | |
| 3-4 = mild to moderate pain | 9 | 20.0% | 25 | 55.6% | 45.7(HS) | <.001 |
| >4 = severe pain | 33 | 73.3% | 2 | 4.4% | | |
| X ± SD | 5.8 ± 1.29 | 2.96 ± 1.13 | t Student test 11.3(HS) | <.001 |
Table 3. Distribution of neonatal pain response parameters in Incubator care group and Kangaroo care group.
| Neonatal pain response parameters | Incubator care group
no=45 | Kangaroo care group
no=45 | | P-value |
| No | % | No | % |
| Facial expression: | | | | | 2.58 ns | >0.05 |
| Relaxed | 3 | 6.7% | 8 | 17.8% |
| Grimace | 42 | 93.3% | 37 | 82.2% |
| Cry: | | | | | 28.9** | <.001 |
| no cry | 6 | 13.3% | 19 | 42.2% |
| Whimper | 14 | 31.1% | 24 | 53.3% |
| vigorous crying | 25 | 55.6% | 2 | 4.4% |
| Breathing patterns: | | | | | 8.78* | < 0.05 |
| Relaxed | 1 | 2.2% | 8 | 17.8% |
| Change in breathing | 44 | 97.8% | 37 | 82.2% |
| Arms: | | | | | 5.29* | < 0.05 |
| Restrained | 1 | 2.2% | 5 | 11.1% |
| Flexed | 44 | 97.8% | 40 | 88.9% |
| Legs: | | | | | 11.25* | < 0.05 |
| Restrained | 1 | 2.2% | 10 | 22.2% |
| Flexed | 44 | 97.8% | 35 | 77.8% |
| State of arousal: | | | | | | |
| Sleeping | 10 | 22.2% | 39 | 86.7% | 37.67** | <.001 |
| awake | 35 | 77.8% | 6 | 13.3% | | |
Table 4. Spearman correlations between total pain score and sex and types of delivery of the studied neonates.
| Sociodemographic characteristics | Total pain score |
| Incubator care group | Kangaroo care group |
| r | P -value | r | P -value |
| Sex | .041 ns | >0.05 | .302* | < 0.05 |
| Types of delivery | -.173-ns | >0.05 | .002 ns | >0.05 |
Table 5. Pearson correlations between total pain score and demographic characteristics of the studied neonates.
| Sociodemographic characteristics | Total pain score |
| Incubator care group | Kangaroo care group |
| r | P -value | r | P -value |
| Gestational age | -.176-ns | >0.05 | -.088-ns | >0.05 |
| Birth weight | .373* | < 0.05 | .142ns | >0.05 |
| Actual weight | .209ns | < 0.05 | .018ns | >0.05 |

Figure 1. Distribution of neonatal respiration in Incubator care group and Kangaroo care.
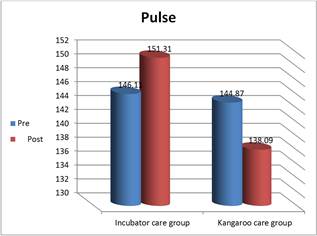
Figure 2. Distribution of neonatal pulse in Incubator care group and Kangaroo care.
5. Discussion
Neonates in the NICU are routinely subjected to various diagnostic, surgical or therapeutic procedures which can result in pain. Numerous clinical studies have demonstrated that failure to treat pain leads to short-term complications and long-term physiological, behavioral, and cognitive impairments. Including altered pain processing, attention deficit disorder impaired visual-perceptual ability or visual-motor integration and poor executive functions [4,29,31]. Conversely, other studies showed needless analgesic therapy prolongs need for mechanical ventilation, delays feeding, or leads to other complications including impaired brain growth, poor socialization skills, and impaired performance in short-term memory tasks [33, 34]. Meanwhile, there was an intense need for nonpharmacological pain management the fragile neonates to avoid any health hazards.
Optimal pain management requires competent pain assessment, which can be especially difficult to perform in neonates [35]. The pain-assessment tool used should be multidimensional, including measurements for both physiologic and behavioral indicators of pain, because neonates cannot self-report. Physiologic indicators of pain include changes in heart rate, respiratory rate, blood pressure, oxygen saturation, vagal tone, palmar sweating, and plasma cortisol or catecholamine concentrations. Behavioral indicators include changes in facial expressions, body movements, and crying [4,26,36].
Consequently, the present study aims to assess the effect of maternal kangaroo care on physiologic measurements and physiologic responses to pain of a heel stick in pre-term neonates. The result of the current study covered five main areas as follows; firstly, socio-demographic characteristic of studied neonates. Secondly, distribution of Physiological measurements of studied groups. Thirdly, distribution of neonatal responses to pain. Fourthly, distribution of neonatal pain response parameters. Lastly, correlations between total pain score and demographic characteristics of the studied neonates.
In relation to distribution of Physiological measurements of studied groups, the study results indicated that, highly statistical significant differences were found between two groups in their pulse and respiration post exposure to painful procedure. This finding comes in agreement with [19] who conducted a study to assess the effect of Kangaroo Care on physiologic responses to pain of an intramuscular injection in neonates. They mentioned that, there were highly significant differences in the mean heart rate, respiratory rate and blood oxygen saturation after minor painful procedure between the KC group and control groups. So, the present study demonstrated that KC given before heel stick minor procedure attenuated the increase in the heart rate and the decrease in respiratory rate which are associated with minor painful procedures.
Regarding, neonatal pain response levels in the studied groups, the current study evident that, the highest percentage of the neonates in kangaroo care group demonstrated no pain, and mild to moderate pain compared to more than three quarters of neonates in incubator care group demonstrated severe level of pain. Also, there was highly statistical significant difference between kangaroo care group and incubator care group in their total pain response score. These findings were in agreement with [42] who reported in a previous study conducted a randomized controlled trial that compared healthy term neonates, 15 of whom were given KC for 10 to 15 minutes before heel stick and remained in KC for the heel stick, to 15 who were swaddled in their crib during a heel stick for routine blood sampling. He found that, the high percentage of neonates in KC group demonstrated mild pain compared to majority of neonates who were swaddled in their crib that demonstrated severe level of pain. Based on the previous results it was obvious that, KC has better effect of alleviating levels of pain in neonates.
In the same context in another study done by Gray et al [43] evaluating the full-term infant’s pain response when heel stick was conducted as the infant lay in KC during breast feeding the findings suggested that, KC considers a form of touch that promotes the infant's ability to moderate the effects of painful factors because KC increases opioid peptide secretion. [44,45]
Concerning the neonatal pain response parameters, the current study proved that highly statistical significant differences were found between kangaroo care group and incubator care group concerning their cry and state of arousal responses to pain from heel stick minor procedure. Also, statistical significant differences were found between two groups regarding their breathing pattern, arms, and legs response to pain. These results come in agreement with Kostandy et al [48] conducted a randomized crossover study on ten preterm neonates with gestational age of 30 to 32 weeks, utilizing either 30 minutes KC or incubator care as the first day intervention and switching to the other intervention on the second day. In this study, Andersen Behavioral Scoring System was used. During the heel stick and recovery phase, there were considerable statistical differences between the two groups. He indicated that, the highly percentage of studied neonates in KC Care group demonstrated whimper cry compared to three quarters of neonates in incubator care who demonstrated vigorous cry.
Moreover, the effect of MKC in reducing pain response in preterm neonates was examined by thirty minutes of KC before and during a heel stick was performed for 74 preterm neonates of 32 to 36 weeks of gestation and compared with incubator care before and during the procedure. Pain severity, as measured by the PIPP, was significantly lower after heel lance in KMC than in incubator care (P < 0.001). This reduction in pain severity was found at 30, 60, and 90 seconds after the procedure. Crying was reduced by 82%, grimacing by 64%, and heart rate increased 8 to 10 bpm in the KC group as compared to 36 to 38 bpm in the swaddled group. Meanwhile the present study evident that, MKC has a better effect on promoting neonatal pain response parameters such as (crying response, breathing pattern. State of arousal and body movements). [49]
As regards to the Pearson correlations between total pain score and demographic characteristics of the studied neonates, this study clarified that, non-statistical significant differences were found between total pain score and demographic characteristics of the studied neonates in both groups where p (>0.05). This result supported by Ludington-Hoe et al. [50, 51] conducted a study on 24 premature neonates. They served as their own controls. One heel stick was performed after the neonate had three hours of KC and the other heel stick was administered after the neonate had been cared in incubator for three hours. This study revealed that, negative correlation was found between total pain score and demographic characteristics of the studied neonates. The mean acceleration rates were 13 and 23 beats per minutes in MKC and incubator groups, respectively.
Finally, and based on the results of the present study MKC reduce neonatal response to pain and improve both physiological and behavioral indicators (pain response parameters) for a safe single painful procedure such as a heel lance.
6. Conclusion
It was concluded that, Kangaroo care had a highly significant effect on neonatal response to pain and their physiological measurements.
Recommendation
1. Kangaroo care should be provided as a routine daily care for all neonates in NICUs. due to its magic effect on infants’ physiological stability and their responses to pain.
2. Further studies are needed to determine whether other caregivers such as fathers, nurses, or siblings could provide similar benefits.
Acknowledgements
We would like to thank the participating mothers and their preterm neonates also, all the NICUs nursing staff.
References
- American Academy of Pediatrics & Canadian Paediatric Society. Prevention and management of pain in the neonate: An update. Pediatrics, (2006). 118(5), 2231- 2241.
- Batton DG, Barrington KJ, Wallman C: Prevention and management of pain in the neonate: an update. Pediatrics. 2007 Feb;119 (2):425.
- Weissman A, Aranovitch M, Blazer S, Zimmer EZ Heel-lancing in newborns: behavioral and spectral analysis assessment of pain control methods. Pediatrics. 2009;124(5):e921.
- Doesburg SM, Chau CM, Cheung TP, Moiseev A, Ribary U, Herdman AT, Miller SP, Cepeda IL, Synnes A, Grunau RE. Neonatal pain-related stress, functional cortical activity and visual-perceptual abilities in school-age children born at extremely low gestational age. Pain.2013;154:1946–52.
- Anand KJS, Palmer FB, Papanicolaou AC. Repetitive neonatal pain and neurocognitive abilities in ex-preterm children. Pain. 2013;154:1899–901.
- Grunau R, Tu MT. Long-term consequences of pain in human neonates. In: Anand KJ, Stevens B, McGrath P, editors. Pain in neonates and Infants. 3rd. Philadelphia, USA: Elsevier Science B.V.; 2007. pp. 45–55.
- Van Hulle, Vincent C. Nurses' knowledge, attitudes, and practices: regarding children’s pain. MCN AM J Matern Child Nurs. 2005; 30(3):177- 83.
- Cong X, Delaney C, Vazquez V. Neonatal nurses' perceptions of pain assessment and management in NICUs: a national survey. Advances in Neonatal Care. 2013;13:353–60.
- Stevens B, Riahi S, Cardoso R, et al. The influence of context on pain practices in the NICU: perceptions of health care professionals. Qualitative Health Research. 2011;21:757–70.
- Ganzewinkel CJ, Anand KJ, Kramer BW, Andriessen P. Chronic Pain in the Newborn: Toward a Definition. Clin J Pain. 2013.
- Guedj R, Danan C, Daoud P, et al.Neonatal pain management is not the same during days and nights in Intensive Care Units: Analysis from the EPIPPAIN Study. British Medical Journal Open. 2014 in press.
- Carbajal R, Nguyen-Bourgain C, Armengaud JB. How can we improve pain relief in neonates? Expert Rev Neurother. 2008;8(11):1617–20.
- Ismail AQ, Gandhi A. Non-pharmacological analgesia: effective but underused. Archives of Disease in Childhood. 2011;96:784–5
- Johnston CC, Stevens B, Pinelli J, et al. Kangaroo Care is effective in diminishing pain response. In Kangaroo Care Annotated Bibliography and References 2015.
- Charpak N, Ruiz JG, Zupan J, Cattaneo A, Figueroa Z, Tessier R, et al.Kangaroo Mother Care: 25 years after. Acta Paediatr. 2005;94(5):514–22.
- Bulfone, G., Nazzi, E., & Tenore, A. (2011). Kangaroo Mother Care and conventional care: A review of the literature. Professioni Infermieristiche, 64(2), 75-82 (ITALIAN). An effective and efficient human care model is Kangaroo Mother Care.
- Cong X, Cusson RM, Walsh S, Hussain N, Ludington-Hoe SM, Zhang D. Effects of skin-to-skin contact on autonomic pain responses in preterm infants. Journal of Pain. 2012;13:636–45.
- Mitchell AJ, Yates CC, Williams DK, Chang JY, Hall RW. Does daily kangaroo care provide sustained pain and stress relief in preterm infants? Journal of Neonatal-Perinatal Medicine. 2013;6:45–52.
- Sajedi, F, Kashaninia Z,, Rahgozar, M, Noghabi, F.A, The Effect of Kangaroo Care on Physiologic Responses to Pain of an Intramuscular Injection in Neonates Iran J Pediatr. Vol 17 (No 4); Pp:339-344.
- Johnston C, Campbell-Yeo M, Fernandes A, Inglis D, Streiner D, Zee R. Skin-to-skin care for procedural pain in neonates. Cochrane Database of Systematic Reviews. 2014.
- Mooncey S, Giannakoulopoulos X, Glover V, Acolet D, Modi N. The effect of mother-infant skin-to-skin contact on plasma cortisol and β-endorphin concentrations in preterm newborns. Infant Behav Develop. 1997;20(4):553–7.
- Johnston CC, Filion F, Campbell-Yeo M, Goulet C, Bell L, McNaughton K, et al. Kangaroo mother care diminishes pain from heel lance in very preterm neonates: a crossover trial. BMC Pediatr. 2008;8:13.
- Conde-Agudelo A, Díaz-Rossello JL. Kangaroo mother care to reduce morbidity and mortality in low birthweight infantsCochrane Database Syst Rev.2014 Apr 22;4:CD002771. doi: 10.1002/14651858.CD002771.pub3.
- Ranger M, Celeste Johnston C, Rennick JE, Limperopoulos C, Heldt T, du Plessis AJ. A multidimensional approach to pain assessment in critically ill infants during a painful procedure. Clinical Journal of Pain. 2013;29:613–20.
- Ganzewinkel CJ, Anand KJ, Kramer BW, Andriessen P. Chronic Pain in the Newborn: Toward a Definition. Clin J Pain. 2013.
- Walden M, Penticuff JH, Stevens B, et al. Maturational changes in physiologic and behavioral responses of preterm neonates to pain. Adv Neonatal Care. 2001;1(2):94-106.
- Grunau R, Tu MT. Long-term consequences of pain in human neonates. In: Anand KJ, Stevens B, McGrath P, editors. Pain in neonates and Infants. 3rd. Philadelphia, USA: Elsevier Science B.V.; 2007. pp. 45–55.
- Dood VL. Implications of kangaroo care for growth and development in preterm infants. J Obstet Gynecol Neonatal Nurs. 2005;34(2):218–232. doi: 0.1177/0884217505274698.
- Maroney DI. Recognizing the potential effect of stress and trauma on premature infants in the NICU: how are outcomes affected? J Perinatol. 2003;23:679–683.
- Rodkey EN, Pillai Riddell R. The infancy of infant pain research: the experimental origins of infant pain denial. J Pain. 2013;14:338–50.
- Bouza, H. (2009). The impact of pain in the immature brain. Journal Maternal Fetal and Neonatal Medicine, 22, 722-732.
- Carbajal R, Chauvet X, Couderc S, Olivier-Martin M. Randomized trial of analgesic effects of sucrose, glucose, and pacifiers in term neonates. BMJ. 1999;319:1393–1397.
- Ferguson SA, Ward WL, Paule MG, Hall RW, Anand KJS. A pilot study of preemptive morphine analgesia in preterm neonates: effects on head circumference, social behavior, and response latencies in early childhood. Neurotoxicol Teratol. 2012;34:47–55.
- de Graaf J, van Lingen RA, Simons SH, et al.Long-term effects of routine morphine infusion in mechanically ventilated neonates on children's functioning: five-year follow-up of a randomized controlled trial. Pain. 2011;152:1391–7.
- Pillai Riddell R, Racine N. Assessing pain in infancy: the caregiver context. Pain Res Manag.2009;14:27–32.
- Johnston CC, Fernandes AM, Campbell-Yeo M. Pain in neonates is different. Pain. 2011;152:S65–73.
- Chermont, A.G., Falcao, L.B., Silva, E.H., Balda, R.C., Guinsburg R.(2009) Skin-to-Skin Contact and/or Oral 25% Dextrose for Procedural Pain Relief for Term Newborn Infants. Pediatrics, 124:6,e1101-e1107.
- Gradin M, Eriksson M, Holmqvist G, Holstein A, Schollin J. Pain reduction at venipuncture in newborns: oral glucose compared with local anesthetic cream. Pediatrics. 2002;110: 1053–1057.
- Ahola Kohut, S., Hillgrove Stuart, J., Stevens, B., Gerwitz-Stern, A. Non-pharmacological management of infant and young child procedural pain. (Review)Cochrane database of systematic reviews (Online)Issue 10, 2011, Pages CD006275.
- Susan M. Ludington-Hoe, Ph.D., Professor andRobert B. Hosseini, M.D. Skin-to-Skin Contact Analgesia for Preterm Infant Heel Stick.Paediatr Child Health 2007;12(2):137-8.
- Ludington-Hoe, Hosseini RB,Torowicz.Skin to skin contact (Kangaroo care)analgesia for preterm infant heel stick AccN.clin Issues,2005,16(3)373-387.
- Gray, L. Watt, L. Blass, E. Skin-to-skin contact is analgesic in healthy newborns. Pediatr. 2000;105(1):e14-24.
- Gray L, Miller LW, Philip BL, et al. Breast feeding is analgesic in healthy newborns. Pediatr.2002;109(4):590-3.
- Weller A, Feldman R. Emotion regulation and touch in infants: the role of cholecystokinin andopioids. Peptides. 2003;24(5):779-88.
- Weller A, Rozin A, Goldstein A, et al. Longitudinal assessment of pituitary-thyroid axis and adrenal function in preterm infants raised by "Kangaroo mother care". Horm Res. 2002; 57(1-2):22-6.
- Castral TC, Warnock F, Leite AM, Haas VJ, Scochi CG. The effects of skin-to-skin contact during acute pain in preterm newborns. Eur J Pain. 2008;12(4):464–71.
- Amin, A., Patel, D, Shah, N., Phatak, A., & Nimblakar, S. (2015- Feb). Report on kangaroo care practices in a tertiary level NICU in Western India – Scope for Improvement. Pediatrcis, 135(Suppl. 1), 58.
- Kostandy RR, Ludington-Hoe SM, Cong X, Abouelfettoh A, Bronson C, Stankus A, et al. Kangaroo Care (skin contact) reduces crying response to pain in preterm neonates: pilot results. Pain Manag Nurs. 2008;9(2):55–65.
- Akcan E, Yigit R, Atici A. The effect of kangaroo care on pain in premature infants during invasive procedures. Turk J Pediatr. 2009;51(1):14–8.
- Ludington-Hoe SM, Hosseini R, Torowicz DL. Skin-to-skin contact (Kangaroo Care) analgesia for preterm infant heel stick. AACN Clin Issues. 2005;16(3):373–87.
- Uvanas-Moberg K, Arn I, Magnusson D. The psychobiology of emotion: the role of the oxytocinergic system. Int J Behav Med. 2005;12(2):59–65.
- Johnston CC, Filion F, Campbell-Yeo M, Goulet C, Bell L, McNaughton K, et al. Kangaroo mother care diminishes pain from heel lance in very preterm neonates: a crossover trial. BMC Pediatr. 2008;8:13.
- Johnston CC, Stevens B, Pinelli J, Gibbins S, Filion F, Jack A, et al. Kangaroo care is effective in diminishing pain response in preterm neonates. Arch Pediatr Adolesc Med. 2003;157(11):1084–8.
- Abouelfettoh A., Ludington-Hoe, S.M., Burant, C., & Visscher, M. (2011). Effect of skin-to-skin contact on preterm infant skin barrier function and hospital-acquired infection. Journal of Clinical Medicine Research, 3(1), 36- 46.
- Mosayebi Z; Javidpour M; Rahmati M; Hagani H; MovahedianAH. The Effect of Kangaroo Mother Care on Pain From Heel Lance in Preterm Newborns Admitted to Neonatal Intensive Care Unit: a Crossover Randomized Clinical Trial. J Compr Ped. 2014 December; 5(4):1-6 e22214.
| Contents |
| |
| |
| 1. | |
| 1.1. | |
| 1.2. | |
| 2. | |
| 2.1. | |
| 2.2. | |
| 2.3. | |
| 2.4. | |
| 3. | |
| 3.1. | |
| 3.2. | |
| 3.3. | |
| 4. | |
| 5. | |
| 6. | |
| |
| |
| |


