| 1. | ||
| 2. | ||
| 3. | ||
| 4. | ||
| 5. | ||
The Cognitive Coping Mechanism and the Quality of Life of the Drug User's Family in Rehabilitation
Iliana Patricia Vega-Campos1, Georgina Olvera-Villanueva2,
Nicolas Padilla-Raygoza3, *
1Master in Nursing Sciences, Academic Unity of Nursing, University Autonomous of Nayarit, Tepic, Mexico
2Doctorate in Nursing Sciences, Departament of Nursing and Obstetrics, Division of Health Sciences and Engineering, Campus Celaya Salvatierra University of Guanajuato, Celaya, Mexico
3Doctorate in Epidemiology, Departament of Nursing and Obstetrics, Division of Health Sciences and Engineering, Campus Celaya Salvatierra University of Guanajuato, Celaya, Mexico
Email address
 (I. P. Vega-Campos)
(I. P. Vega-Campos)  (G. Olvera-Villanueva)
(G. Olvera-Villanueva)  (N. Padilla-Raygoza)
(N. Padilla-Raygoza)  (N. Padilla-Raygoza)
(N. Padilla-Raygoza) Citation
Iliana Patricia Vega-Campos, Georgina Olvera-Villanueva, Nicolas Padilla-Raygoza. The Cognitive Coping Mechanism and the Quality of Life of the Drug User's Family in Rehabilitation. Journal of Nursing Science. Vol. 2, No. 6, 2016, pp. 39-46.
Abstract
The objective was determine the relationship between the effect and impact of cognitive coping mechanism and quality of life of the family member with drug user rehabilitation, in Tepic, Nayarit, Mexico. The study was a cross-sectional, analytic study; sample consisted of 68 families, who signed the informed consent, the questionnaire Cognitive Coping Mechanisms and Quality of Family Life questionnaires were used. In the sample was found association between compromised cognitive coping mechanism and compromised quality of family life (X2 = 7.64, df = 1, p <0.05), strong effect (OR = 6.94 95%CI = 1.40 to 34.37); and impact of AFe = 85.59%. Adjusted for marital status, OR = 10.33. The main conclusion was: The family of the drug user rehabilitation has a compromised quality of life when cognitive coping mechanisms are compromised.
Keywords
Drug Dependence, Cognitive Coping Mechanisms, Quality of Life, Rehabilitation
1. Introduction
The World Health Organization (WHO) points to drug use as one of the most important problems facing society, because of the magnitude of the phenomenon and because of the personal and social consequences derived from it; it is noted that 4.8% of the world's population consumes some type of drug, therefore there are many families affected by this event. [1]
According to the United Nations (UN), there are 185 million drug users in the world, representing 4.5% of the population over 15 years of age. In Mexico, the proportion of drug users compared to the world population, for each 2.5 drug users in the world there is one in Mexico. [2]
The Epidemiological Surveillance System in Addictions (SISVEA), as part of one of its strategies, collects information from governmental and non-governmental institutions that deal with the problem of addictions and this has allowed documenting the overview of the phenomenon of drug use in the country. SISVEA reported in 2008 that the state of Nayarit has six rehabilitation centers and a juvenile guardianship council. Of the population that goes to rehabilitation centers, 65.2% is due to alcohol, 5.6% from intravenous drug use, and the remaining 29.2% from cocaine and marijuana use. [3]
Once the drug addiction in a family member is presented and the rehabilitation process is necessary, it causes emotional, economic and social devastation in the family, since they are not prepared to live in this phenomenon and put at risk the quality Family life.
It is here that nurses can intervene with actions aimed at improving the quality of life of the family, which is one of its main objectives.
Roy considers that the person-family has two mechanisms to achieve adaptation: the regulator and the cognitive. The latter responds through four cognitive-emotive channels, which are perceptive, learning, judgment and emotion. The perceptive includes mental activities such as attention, coding and selective memory, learning implies imitation and reinforcement and integration. Judgment encompasses problem-solving and decision-making activities, while emotions include feelings, elements that are necessary to have adaptive responses to family risk factors. Adaptive responses are those that promote the integrity of the human system in terms of the goals of adaptation, survival, reproduction, reproduction and transformations of the person and the environment. [4]
Roy mentions that the cognitive coping mechanism responds to stimuli through effective and ineffective responses [4]; this mechanism in families with a sick member has ineffective responses in some or all of the channels which causes a risk in the quality of life of the family.
Mora Antó et al., described the quality of life characteristics of adults with intellectual disabilities in Colombia; it was found that the family first lacks information, but at the same time there is cohesion, but this appears as a mechanism of survival and a resigned attitude; in addition to lacking psychosocial support; the situation is complex because the members with intellectual disability end up affecting the family and the family does not have the necessary resources and does not identify them, since they do not conceive of the demands that must be fulfilled which results in a compromised level of quality of life. [5]
Studying the disability of a member in the family and the quality of life of the family, it assumes that the disease will have a high impact in all the group and will modify the interrelation established between the different members of the same; it is possible that it affects the professional and time relationships to carry out social and recreational activities, there will be greater burden, isolation, together will generate a mismatch and their quality of life changes and although the adaptation of the family often depends on the type of illness Having the affected member. [6]
The relatives of a person with a mental disorder must face the emotional burden of caring for the patient, supporting him financially if he does not work, covering the costs of care; It is also necessary to consider the time that some family members must stop working, and therefore, not to receive economic income with the corresponding repercussions in the reduction of the quality of life in the family. [7]
It has been observed that families who have a drug user member in rehabilitation face a large number of negative stimuli, causing their cognitive coping mechanism in their channels of perception, learning, judgment and emotions to have ineffective responses to this health situation. [8]
The emotional climate produced by attempts to control the behavior of the addict is mainly stress, because the drug user increases their dependency and the family concentrates on avoiding consumption and abuse. Because the family cannot change the behavior of the addict, the family presents feelings of frustration, guilt and depression, embarrassment and inability to make decisions, which leads to a logical consequence of their quality of life being compromised in terms of physical well-being, social integration / social inclusion. [8]
Commonly, it is believed that the one who needs help is the patient identified with drug dependence; but the reality is that all members of the family need help, because they also suffer indirectly the disease and need a whole process of rehabilitation towards health.
Thus, a process of passive acceptance is developed in the family that is conforming to the fact that things are like that and cannot be changed. This feeling of impotence generates more and more emotional suffering, sustains the confusion of roles and bad intra-family and social relationships.
The compromise (deterioration) of the quality of life is one of the most serious consequences for the family with a drug user in rehabilitation. Cognitive and behavioral effort is constantly being modified to try to meet emotional, social and economic demands.
Internment for drug rehabilitation is still currently stigmatized, and it may be difficult for the family to confront it with their community. Instead, it is preferable to evade the events surrounding the event, to isolate oneself and to break the bonds that previously had with the extended family, with friends, or neighbors.
Therefore, it is intended to identify the relationship between the cognitive coping mechanism and the quality of life of the drug user's family in rehabilitation.
2. Material and Methods
The study was reviewed and approved by Bioethics Committee of Division of Health Sciences and Engineering, Campus Celaya-Salvatierra, University of Guanajuato, Mexico.
Study design. It was cross-sectional, observational, analytic.
Study place. Rehabilitation Center in Tepic, Nayarit, Mexico.
Selection of families.
Inclusion criteria.
To be a parent, spouse or guardian of a drug user with a maximum period of 2 months in the Rehabilitation Center and who agreed to participate in the study, signing the informed consent.
Exclusion criteria
Who did not accept to participate.
Variables
Sociodemographics
It was measure age, gender, education, occupation, marital status and family relationship to the drug user in rehabilitation.
Independent
Cognitive coping mechanisms (CCM), is a dichotomic categorical variable; it is the way an individual faces a situation; it is measured as compromised or compensated / integrated through Cognitive Coping Mechanism Questionnaire and include three-dimensions: learning, judgment and emotions; it was present with frecuencies and percentages.
Outcome
Quality of family life (QFL) is a dichotomic categorical variable; it is the physical, emotional, and social well-being of the family, including the dimensions: interpersonal relationships, physical well-being, social inclusion, measured as compromised or compensated/integrated; it was present with frequencies and percentages.
Instruments
To measure the cognitive coping mechanism, was used the cognitive coping mechanism questionnaire (CCMQ) [9] modified for this study. The instrument consists of 9 questions with Likert scale responses with 5 options, total score of 9 to 45, meaning that the score of 9 to 20 CCM are compromised, 21 to 32 are compensated and 33 to 45 integrated. We obtained an overall reliability of 0.91 of Cronbach's alpha, 0.89 for the learning dimension, 0.91 for the judgment dimension and 0.86 for the dimension emotions. For learning, judgment and emotions the scores were 3 to 15 for each of the dimensions considering 3 to 6 compromised, 7 to 11 compensated, 12 to 15 integrated.
Regarding quality of life, the quality family life questionnaire (QFLQ) [10] was used, consisting of 8 questions with Likert type scale answers, with 5 options, being able to obtain a score between 8 and 40. Score 8 to 18 the QFLQ is compromised, 19 to 29 compensated and 30 to 40 is integrated. It had Cronbach alpha of 0.89 global, 0.75 interpersonal relationships, 0.72 social integration and 0.89 physical well-being of the family. Interpersonal relationships consists of 2 questions with scores between 2 and 10 (score 2 to 4 compromised, 5 to 7 compensated, 8 to 10 integrated); Social integration consists of 3 items with scores of 3 to 15 (3 to 7 compromised, 8 to 12 compensated, 13 to 15 integrated) and the same for the dimension of family physical well-being (3 to 7 compromised, 8 to 12 compensated, 13-15).
Sample size
Assuming that 55% of the participants have CCM compromised and 15% with CCM compensated, both with compromised QFL, the minimum sample size is 15 in the compromised CCM group and 30 in the compensated CCM group, with 95% accuracy and 80% power (EpiInfo 7.0, 2013, CDC, Atlanta, GA, USA).
Statistical analysis
For the demographic variables, descriptive statistics were used, means and standard deviations for quantitative variables and frequencies and percentages for qualitative variables; to demonstrate an association between CCM and QFL was used Chi-squared test and p value. In order to measure the effect of CCM on QFL, was calculated Odds Ratio (OR) and Attributable Fraction on Exposed (AFe) was calculated to measure impact.
A logistic regression model was generated between CCM and QFL with the demographic variables, to demonstrate confusion and / or effect modification.
To demonstrate statistical significance of the results p-value was fixed at 0.05.
Statistical analysis was performed on STATA 13.0® (STATA Corp., College Station, TX, USA).
3. Results
The sample consisted of 68 family members of drug users admitted to rehabilitation centers. Their age range was 18 to 74 years, with a mean of 43.57 ± 16.59 years and the number of relatives at home ranged from 2 to 9 with a mean of 4.78 ± 1.20 family members.
The demographic characteristics of the participants is shown in Table 1, predominantly women, spouse, married, housewives with elementary schooling finished, and housekeeper.
Table 1. Sociodemographic characteristics of user drug’s family, Tepic.
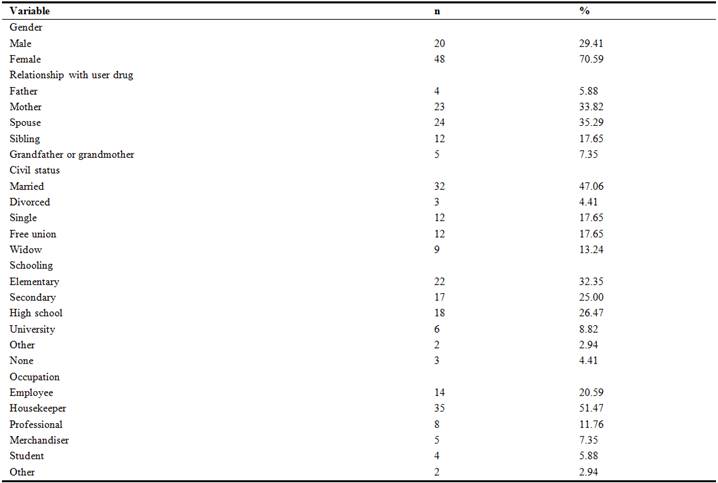
Source: Study forms
Table 2 shows the tabulation between CCM and QFL, where an association was demonstrated (p <.05) and families with compromised QFL were almost 7 times more likely to have CCM compromised. According to AFe, 85.59% of families with compromised QFL would have been avoided if the CCM had been compensated or integrated.
Table 2. Tabulation among Cognitive Coping Mechanism and Quality Family Life, Tepic.

C= compromised, C/I= compensated/integrated OR= Odds Ratio, CI95%= Confidence intervals at 95%, AFe= Attributable Fraction in Exposed
df=degree of freedom
Source: Cognitive Coping Mechanism Questionnaire and Quality Family Life Questionnaire
When generating the logistic regression model, only civil status shows characteristics to be considered as confounders. When adjusted for civil status the OR increased to 10.33.
There is no evidence that civil status causes interaction because when stratified by civil status, Chi square for homogeneity was 3.01 with 2 degrees of freedom and p-value of 0.22. Occupation and gender were not considered as confounders (p> 0.05).
The dimensions of CCM with QFL were tabulated, and it was found that there is a statistically significant association between learning and QFL (p <.05) and families with QFL compromised were 5 times more likely to have compromised learning compared to families who had compensated or integrated QFL; in addition, 80% of families with compromised QFL would have been avoided if learning had been compensated or integrated (Table 3).
The association between judgment and QFL was statistically significant (p <.05) and families with QFL compromised were 6.5 times more likely to have impaired judgment compared to families with compensated or integrated QFL; in addition, 85.29% of families with compromised QFL would have been avoided if the judgement was compensated / integrated (Table 3).
The association between emotions and QFL is statistically significant (p <.05); and families with compromised QFL were 6.5 times more likely to have compromised emotions compared to families with compensated or integrated QFL; 85% of families with compromised QFL would have been avoided if the emotions were compensated or integrated (Table 3).
Table 3. Tabulation between dimensions of cognitive coping mechanisms and the quality of family life of the drug user, Tepic.
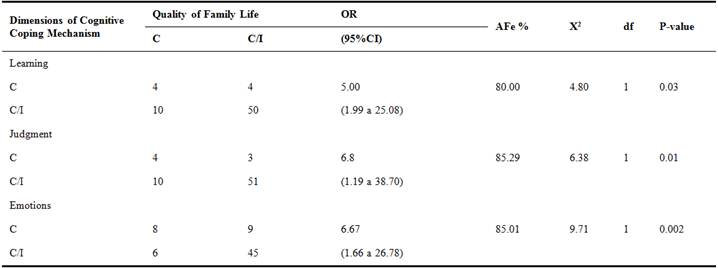
C=Compromised C/I=Compensated/integrated, OR= Odds Ratio, CI95%= Confidence Intervals at 95%, AFe=Attributable Fraction in Exposed, df= degree of freedom
Source: Cognitive Coping Mechanism Questionnaire and Quality of Family LIfe Questionnaire
In the tabulation of CCM with the QFL dimensions, it was found that there was no association of CCM with interpersonal relationships (p>.05) or social integration (p>.05); There was a statistically significant association between CCM with family well-being (p <.05) and those with compromised family well-being were more than 5 times more likely to have CCM compromised compared to families with compensated or integrated well-being and 81.41% of families with compromised well-being would have been avoided if the CCM had been compensated or integrated (Table 4).
Table 4. Tabulation between cognitive coping mechanism and family quality of life dimensions, Tepic.
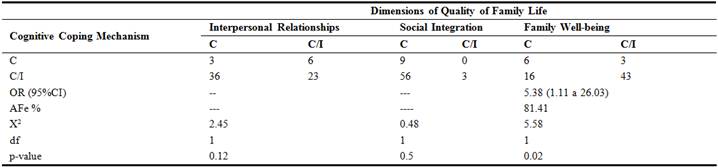
C=Compromised C/I=Compensated/integrated, OR= Odds Ratio, CI95%= Confidence intervals at 95%, AFe=Attributable fraction in exposed, df= degree of freedom
Source: Cognitive Coping Mechanism Questionnaire and Quality Family Life Questionnaire
In the tabulation between dimensions and CCM and dimensions of QFL dimensions, we found a statistically significant association between learning (CCM) and family well-being QFL (p <.05) and between emotions (CCM) and family well-being QFL (p<.05) (Table 5).
Table 5. Tabulation between dimensions of cognitive coping mechanism and dimensions of the quality of family life, Tepic.
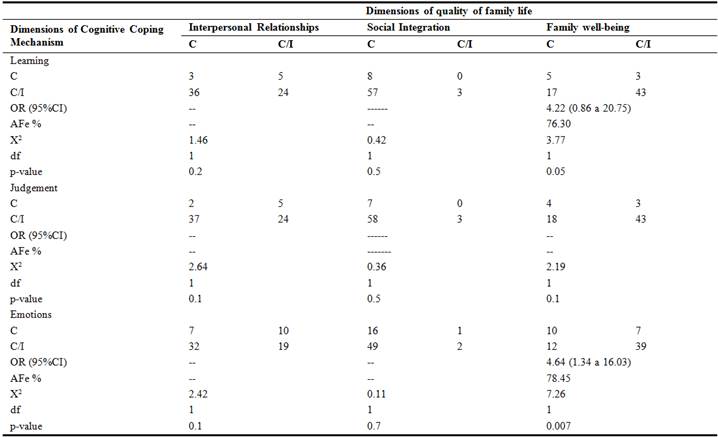
C=Compromised C/I=Compensated/integrated OR= Odds Ratios, CI95%= Confidence intervals at 95%, AFe=Attributable fraction in exposed, df= degree of freedom
Source: Cognitive Coping Mechanism Questionnairte and Quality Family Life Questionnaire
4. Discussion
In the face of serious illness as a stressful stimulus, which includes sudden, immediate or unpredictable changes in lifestyle, ambiguous situations, life-threatening alterations or limitations, people develop behaviors and thoughts known as coping situation. [11]
One strength of the study was that it was possible to study the universe of relatives who had a family member hospitalized in the rehabilitation center.
The research aimed to demonstrate how the relationship and effect and impact that exists between the mechanisms of cognitive coping and the quality of life of the family with a drug user member in rehabilitation, considering this experience as an event that conditions stimuli in which activates the coping mechanisms described by Roy in his Adaptation Model.
It is not easy to live with a drug user in the process of rehabilitation, it is understood that for the relatives, there is a predisposition to not believe in the treatment.
Together, the large inter-individual variability that has been observed in the study, reveal that when talking about family in general, it is very difficult to identify, if there are stereotypes and / or categories of families. It is possible to indicate that the high interindividual variability of the results of our work may be due to the measurement instrument used. [12]
Mora Antó et al., reported that 48.9% of families with an adult with intellectual disability in Colombia, expressed satisfaction with their quality of life [5]; in this sample in Mexico, it was found that 22% are at a compromised level, 71% at the compensatory level and only 7% at an integrated level and in the quality of family life.
The families studied present a great deal of stimulus towards the coping subsystems, which alter the adaptive modes, constituting a risk of ineffective adaptive responses which results in a potential risk to their health, finding that within these scores can be broken down each dimension of quality of life finding in interpersonal relationships 56% is compromised, in the dimension of social inclusion 76% of find in the category of compensatory and finally for the dimension of physical well-being 57% in compensatory level; indicating that the major problem with quality of life is in the channel-dimension of interpersonal relationships, which may be affecting the other channels.
These risks raise the demands of everyday life and place the family in a situation of overexertion to cope with a member's drug rehabilitation situation, making use of each channel of cognitive coping mechanisms to try to provide effective responses.
15% of the families investigated were found to be at a compromised level of cognitive coping mechanisms, while 51% were at a compensatory level, which is an expression of ineffective adaptive responses. These families develop a daily life with high demands and also dysfunctional; their dysfunctionality does not allow for cohesion (interpersonal relationships), the realization of role change, nor the flexibility of norms, which means that their capacity for adaptability is limited. The negative manifestation of the relational processes within it restricts the fulfillment of the basic functions that as a human system must fulfill with its members.
As the health of a member of these families is compromised, they maintain an unadjusted behavior in the face of contingency, such as rehabilitation for drug use, which makes them specialized candidates for intervention, as well as the patient drug user who is under treatment.
The results of this investigation differ from those obtained in others. For example, in the study carried out by Louro, "Theoretical-methodological model for the evaluation of family health in primary care", identified that 51% are in an integrated condition or in the process of adaptation and 6.1% in a serious level of affectation of family health.[13]
Also in the study by Dejo Vásquez, "A sense of coherence, coping and overload in family caregivers of elderly people with chronic disease" identified that the female gender is predominant; while an inverse relationship between coping strategies and coherence was found. [14]
The comparison with these results leads to the analysis that the integral diagnosis on the health situation of the families studied in the research presented does not have a behavior similar to that performed for other families. The difference lies in the fact that for the first time instruments were applied exclusively in families that have a member of drug users in rehabilitation and this element prints a stamp of distinction.
It is evident that the family of the drug-dependent patient has problems of adaptation, since the stimuli that influence in the behavior surpass the capacity of coping. When ineffective behavior is identified, it is indisputable that these coping processes were not able to effectively adapt to the stimulus it was affecting. In this case the stimulus is the process of rehabilitation of a relative, affecting the quality of life of the whole family.
This study confirms the approaches of Lazarus and Folkman [15] on the strategies identified in the study participants; individuals employ two general types of strategies, problem solving, directly directed to manage or alter it, and those of emotional regulation, through methods aimed at regulating the emotional response to the problem.
Another problem is the stigmatization and discrimination suffered by drug users in Mexico, as Mora-Rios et al. [16] reported, and it is another factor that would affect the quality of life of the drug user's family in rehabilitation.
It is important to design intervention strategies, to improve family coping, that a member of the family is a drug user, as reported by Bisetto et al. [17], where they applied an intervention to the family, improving the self-esteem, decreasing anxiety and anger state.
5. Conclusions
The findings allow us to express that nursing research based on self-knowledge strengthens the autonomy of nursing staff and contributes to improving the care given in all contexts.
Disorders due to drug use generate a huge burden on the family, causing large-scale interpersonal conflicts, inappropriate behavior, and affecting the quality of life of the whole family.
It is evident that the family of the drug user has problems of adaptation referring to their quality of life, since the stimuli that influence the behavior or the capacity to cope with the stimuli of the environment activates the processes of coping to produce behaviors. It is concluded that this study offers two useful and important considerations, the first is that in general families undergoing a process of rehabilitation of a drug user member, their quality of life decreases and that this decrease is more noticeable in women than in men, the second is that coping mechanisms during rehabilitation treatment does not seem to depend on variables such as sex and age. Therefore, to determine the characteristics that would define the profile of the family that goes through a process of rehabilitation of a member is necessary to resort to the valuation of other aspects. Each family in particular constitutes something unique, and therefore the determination of its characteristics and the type of support that can be most beneficial to it is something that must be carried out by means of a complete evaluation that integrates, along with the psychological aspects, those other derivatives directly from your medical family history. The nursing role is directed towards the identification of needs of the cognitive subsystem, generating specific diagnoses of the discipline that allow to determine strategies of intervention to achieve the adaptation of the person-family to critical situations such as drug addiction; this in order to promote adaptation.
The above considerations constitute a contribution to the development of Roy's Model of Adaptation, since it can be used by nursing professionals interested in knowing the relationship of coping mechanisms and the quality of life of the family, in order to effectively address the Nursing care.
It is recommended to continue the research to establish the relationship between the different variables and coping and adaptation capacity, as well as the design of nursing care plans aimed at identifying coping strategies in families.
It reports findings, which relate the mechanisms of coping and the quality of life perceived, carried out in our environment, which lead us to value and consider, that coping is one of the fundamental determinants of value judgment of the quality of life, and its possible link with the self-assessment, both considered regulatory mechanisms that allow the adaptation of the individual and his environment.
It must be very careful with the data obtained in the comparisons between the female and male gender, since the female gender is greater than the male gender among the sample. For this reason it is considered important to do studies with larger samples. In addition, it is convenient to carry out studies using structured or semi-structured interviews to evaluate the family and obtain more information than the one provided by the instrument used.
In spite of the above limitations, it has been considered necessary to carry out this work to take into account a multidimensional approach on the referred variables in a group as homogeneous as possible of families that can be used to find guidelines for future research and to develop interventions of Nurses to these families. Trying to evaluate so many dimensions in this study group is a very complex but necessary task facing a multidisciplinary approach.
It is necessary for the nursing professional to establish their own interventions based on the behavior and specific stimuli that are identified in the family through the care process, since this professional is responsible for inspecting and helping the family to recognize the negative focal stimuli that make it difficult for the family to have an effective adaptive response in their quality of life.
References


